Ipratropium bromide, salbutamol.
1 unit-dose vial (2.5 ml) Nebuliser solution contains (8r)-3α-hydroxy-8-isopropyl-1αH,5αH-tropanium bromide (±)-tropate monohydrate (= ipratropium bromide) corresponding to 0.5 mg ipratropium bromide anhydrous 520 mcg, di[(RS)-2-tert-butylamino-1-(4-hydroxy-3-hydroxymethyl-phenyl)ethanol] sulphate (= salbutamol sulphate) corresponding to 2.5 mg salbutamol base 3010 mcg.
Excipients/Inactive Ingredients: sodium chloride, hydrochloric acid, purified water.
Pharmacotherapeutic group: Adrenergics in combination with anticholinergics for obstructive airway diseases. ATC code: R03AL02.
PHARMACOLOGY: Mode of Action: Ipratropium bromide is a quaternary ammonium compound with anticholinergic (parasympatholytic) properties. In nonclinical studies, it appears to inhibit vagally mediated reflexes by antagonizing the action of acetylcholine, the transmitter agent released from the vagus nerve. Anticholinergics prevent the increase in intracellular concentration of Ca++ which is caused by interaction of acetylcholine with the muscarinic receptor on bronchial smooth muscle. Ca++ release is mediated by the second messenger system consisting of IP3 (inositol triphosphate) and DAG (diacylglycerol).
Pharmacodynamics: The bronchodilation following inhalation of ipratropium bromide is primarily local and site specific to the lung and not systemic in nature.
Salbutamol sulphate is a beta2-adrenergic agent which acts on airway smooth muscle resulting in relaxation. Salbutamol relaxes all smooth muscle from the trachea to the terminal bronchioles and protects against all bronchoconstrictor challenges.
COMBIVENT provides the simultaneous release of ipratropium bromide and salbutamol sulphate allowing the additive effect on both muscarinic and beta2-adrenergic receptors in the lung resulting in a bronchodilation which is superior to that provided by each single agent.
Clinical Trials: Controlled studies in patients with reversible bronchospasm have demonstrated that COMBIVENT has a greater bronchodilator effect than either of its components and there was no potentiation of adverse events.
Pharmacokinetics: From a pharmacokinetic perspective, the efficacy observed in the COMBIVENT pressurised inhalation, suspension pulmonary clinical trials is due to a local effect on the lung following inhalation.
Following inhalation 10 to 39% of a dose is generally deposited in the lungs, depending on the formulation, inhalation technique and device, while the remainder of the delivered dose is deposited in the mouthpiece, mouth and the upper part of the respiratory tract (oropharynx).
The portion of the dose deposited in the lungs reaches the circulation rapidly (within minutes). The amount of the active substance deposited in the oropharynx is slowly swallowed and passes the gastrointestinal tract. Therefore the systemic exposure is a function of both oral and lung bioavailability.
Coadministration of ipratropium bromide and salbutamol sulphate does not potentiate the systemic absorption of either component and therefore the additive activity of COMBIVENT is due to the combined local effect on the lung following inhalation.
Ipratropium: Absorption: Cumulative renal excretion (0-24 hrs) of ipratropium (parent compound) is below 1% of an oral dose and approximately 3-13% of an inhaled dose. Based on these data, the total systemic bioavailability of oral and inhaled doses of ipratropium bromide is estimated at 2% and 7 to 28% respectively. Taking this into account, swallowed dose portions of ipratropium bromide do not relevantly contribute to systemic exposure.
Distribution: Kinetic parameters describing the disposition of ipratropium were calculated from plasma concentrations after i.v. administration. A rapid biphasic decline in plasma concentrations is observed. The apparent volume of distribution at steady-state (Vdss) is approximately 176 L (≈ 2.4 L/kg). The drug is minimally (less than 20%) bound to plasma proteins. Nonclinical data indicate that the quaternary amine ipratropium does not cross the placental or the blood-brain barrier.
The main urinary metabolites bind poorly to the muscarinic receptor and have to be regarded as ineffective.
Biotransformation: After intravenous administration approximately 60% of a dose is metabolised the major portion probably in the liver by oxidation.
Elimination: The half-life of the terminal elimination phase is approximately 1.6 hours. Ipratropium has a total clearance of 2.3 L/min and a renal clearance of 0.9 L/min. In an excretion balance study cumulative renal excretion (6 days) of drug-related radioactivity (including parent compound and all metabolites) accounted for 9.3% after oral administration and 3.2% after inhalation. Total radioactivity excreted via the faeces was 88.5% following oral dosing and 69.4% after inhalation. The half-life for elimination of drug-related radioactivity (parent compound and metabolites) is 3.6 hours.
Salbutamol: Absorption and Distribution: Salbutamol is rapidly and completely absorbed following oral administration either by the inhaled or gastric route and has an oral bioavalability of approximately 50%. Mean peak plasma salbutamol concentrations of 492 pg/mL occur within three hours after inhalation of COMBIVENT. Kinetic parameters were calculated from plasma concentrations after i.v. administration. The apparent volume of distribution (Vz) is approximately 156 L (≈ 2.5 L/kg). Only 8% of the drug is bound to plasma proteins. In nonclinical trials, levels of approximately 5% of the plasma level of salbutamol are found in the brain. However, this amount probably represents the distribution of the substance in the extracellular water of the brain.
Biotransformation and Elimination: Following this single inhaled administration, approximately 27% of the estimated mouthpiece dose is excreted unchanged in the 24-hour urine. The mean terminal half-life is approximately 4 hours with a mean total clearance of 480 mL/min and a mean renal clearance of 291 mL/min.
Salbutamol is conjugatively metabolised to salbutamol 4'-O-sulphate. The R(-)-enantiomer of salbutamol (levosalbutamol) is preferentially metabolised and is therefore cleared from the body more rapidly than the S(+)-enantiomer. After oral administration urinary excretion of unchanged drug and sulphate conjugate were 31.8% and 48.2% of the dose, respectively.
TOXICOLOGY: Single-dose toxicity: The acute toxicity of COMBIVENT after single inhalation administration was tested in rats and dogs. Up to the highest technically feasible dose (rat: 887/5397 mcg/kg ipratropium bromide/salbutamol, dog: 164/861 mcg/kg ipratropium bromide/salbutamol) there were no indications of systemic toxic effects, the combination was locally well tolerated. The approximate LD50 after intravenous administration was calculated for the individual substances to be between 12 and 20 mg/kg for ipratropium bromide and between 60 and 73 mg/kg for salbutamol sulphate depending on the species tested (mouse, rat, dog).
Repeat-dose toxicity: Two 13-week inhalation toxicity studies in rats and dogs have been performed with the combination of ipratropium bromide and salbutamol sulphate. In these studies, the heart proved to be the target organ. In the rat at dosages of 34/197 to 354.5/2604 mcg/kg/day ipratropium bromide/salbutamol sulphate, a non dose dependent increase in heart weights was present, however without any histopathological correlate. In the dog at doses of 32/198 to 129/790 mcg/kg/day ipratropium bromide/salbutamol sulphate, slightly increased heart rates and, at higher dosages, histopathologically detectable scars and/or fibrosis in the papillary muscle of the left ventricle, sometimes accompanied with mineralisation, were observed.
The cardiovascular findings obtained in the previously mentioned studies must be regarded as well known effects of beta-adrenergics such as salbutamol. The toxicological profile of ipratropium bromide is also well known for many years and characterised by typical anticholinergic effects as dryness of the mucosal membranes of the head, mydriasis, keratoconjunctivitis sicca (dry eye) in dogs only, reduction in tone and inhibition of motility in the gastrointestinal tract (rat).
Reproduction toxicity: Reproduction toxicity studies are available for the two individual components of COMBIVENT. Salbutamol sulphate caused cleft palates at high subcutaneous dosages in mice, starting at dosages in the range of the inhalation MRHDD (based on mg/m2). However this phenomenon is well known and occurs also after the administration of other beta-adrenergic compounds. Today it is assumed that this effect is caused by an increase in the maternal corticosterone level and might be regarded as a result of general stress not relevant for other species. Apart from these findings, the studies performed with salbutamol sulphate and with ipratropium bromide revealed only marginal effects, if any, on embryos, foetuses and pups and these only in the range of maternal toxicity. Ipratropium bromide did not affect fertility of male or female rats at oral doses up to 50 mg/kg (approximately 3,400 times the MRHDD on a mg/m2 basis). Reproduction studies in rats with salbutamol revealed no evidence of impaired fertility.
Genotoxicity: Both individual substances were tested in numerous in-vivo and in-vitro genotoxicity tests. Neither salbutamol sulphate nor ipratropium bromide showed any evidence of mutagenic properties. In addition COMBIVENT did not show genotoxic activity in in vitro assays.
Carcinogenicity: Salbutamol sulphate and ipratropium bromide were tested individually for neoplastic properties in several carcinogenicity studies. After oral administration of salbutamol sulphate in rats, but not in mice, hamsters and dogs, an increased incidence of leiomyomas of the mesovarium was observed at dosages about ≥20-fold higher than inhalation MRHDD. The development of the leiomyomas was found to be preventable by simultaneous administration of beta-blockers. These findings were assessed to be species specific and therefore without clinical relevance, consequently not leading to any restriction of the clinical use of salbutamol sulphate.
Ipratropium bromide revealed no carcinogenic potential when tested orally in mice and rats.
Immunogenicity: No evidence was found of any immunotoxicological effect caused by COMBIVENT or its individual active ingredients.
COMBIVENT is indicated for the management of reversible bronchospasm associated with obstructive airway diseases in patients who require more than a single bronchodilator.
Patients should be advised to consult a physician or the nearest hospital immediately in the case of acute or rapidly worsening dyspnoea if additional inhalations of COMBIVENT do not produce an adequate improvement.
If higher than recommended doses of COMBIVENT are required to control symptoms, the patient's therapy plan should be reviewed.
In asthma, concomitant anti-inflammatory therapy should be considered.
Dosage: The following doses of COMBIVENT are recommended for adults (including elderly patients).
COMBIVENT nebuliser solution in unit dose vials may be administered from a suitable nebuliser or an intermittent positive pressure ventilator.
Treatment should be initiated and administered under medical supervision, e.g. in the hospital setting. Home based treatment can be recommended in exceptional cases (severe symptoms or experienced patients requiring higher doses) when a low dose rapid acting beta-agonist bronchodilator has been insufficient in providing relief after consultation with an experienced physician.
The treatment with the nebuliser solution in UDVs should always be started with the lowest recommended dose (1 UDV). In very severe cases two unit dose vials may be required for symptom relief. Administration should be stopped when sufficient symptom relief is achieved.
Treatment of acute attacks: 1 unit dose vial is sufficient for prompt symptom relief in many cases.
In severe cases if an attack has not been relieved by one unit dose vial, the administration of a second unit dose vial may be required. Patients should be advised to consult the physician or the nearest hospital immediately in these cases.
Maintenance treatment: 1 unit dose vial three or four times daily.
SPECIAL POPULATIONS: Patients with hepatic or renal impairment: COMBIVENT has not been studied in patients with hepatic or renal insufficiency. It should be used with caution in those patient population.
Paediatric population: Because of insufficient information in children COMBIVENT is not indicated for paediatric patients.
INSTRUCTIONS FOR USE/HANDLING: The unit dose vials are intended only for inhalation with suitable nebulising devices and must not be taken orally or administered parenterally.
The content of the unit dose vials does not need to be diluted for nebulization.
1. Prepare the nebuliser for filling, according to the instructions provided by the manufacturer or physician.
2. Open the pouch foil and tear one unit dose vial from the strip.
3. Open the unit dose vial by firmly twisting the top.
4. Squeeze the content of the unit dose vial into the nebuliser reservoir.
5. Assemble the nebuliser and use as directed.
6. After use throw away any solution left in the reservoir and clean the nebuliser, following the manufacturer's instructions.
Since the unit dose vials contain no preservative, it is important that the contents are used soon after opening and that a fresh vial is used for each administration to avoid microbial contamination. Partly used, opened or damaged unit dose vials should be discarded.
It is strongly recommended not to mix COMBIVENT nebuliser solution with other drugs in the same nebuliser.
Symptoms: The effects of overdosage are expected to be primarily related to salbutamol.
The expected symptoms with overdosage are those of excessive beta-adrenergic-stimulation, the most prominent being tachycardia, palpitation, tremor, hypertension, hypotension, hypokalaemia, widening of the pulse pressure, anginal pain, arrhythmias, and flushing. Metabolic acidosis has also been observed with overdosage of salbutamol.
Expected symptoms of overdosage with ipratropium bromide (such as dry mouth, visual accomodation disorders) are mild and transient in nature in view of the wide therapeutic range and topical administration.
Therapy: Treatment with COMBIVENT should be discontinued. Acid base and electrolyte monitoring should be considered.
Administration of sedatives, and in severe cases intensive therapy may be needed.
Beta-receptor blockers, preferably beta1-selective, are suitable as specific antidotes; however, a possible increase in bronchial obstruction must be taken into account and the dose should be adjusted carefully in patients suffering from bronchial asthma.
COMBIVENT is contraindicated in: Patients with hypertrophic obstructive cardiomyopathy or tachyarrhythmia.
Patients with known hypersensitivity to atropine or its derivatives or to any other component of the product.
Hypersensitivity: Immediate hypersensitivity reactions may occur after administration of COMBIVENT, as demonstrated by rare cases of urticaria, angioedema, rash, bronchospasm and oropharyngeal oedema.
Paradoxical bronchospasm: As with other inhaled medicines COMBIVENT may result in paradoxical bronchospasm that may be life-threatening. If paradoxical bronchospasm occurs COMBIVENT should be discontinued immediately and substituted with an alternative therapy.
Ocular complications: There have been isolated cases of ocular complications (i.e. mydriasis, increased intraocular pressure, narrow-angle glaucoma, eye pain) when aerosolised ipratropium bromide either alone or in combination with an adrenergic beta2-agonist, has come in contact with the eyes.
Eye pain or discomfort, blurred vision, visual halos or colored images in association with red eyes from conjunctival congestion and corneal oedema may be signs of acute narrow-angle glaucoma. Should any combination of these symptoms develop, treatment with miotic drops should be initiated and specialist advice sought immediately.
Patients must be instructed in the correct administration of COMBIVENT. Care must be taken not to allow the solution or mist to enter into the eyes. Patients who may be predisposed to glaucoma should be warned specifically to protect their eyes.
It is recommended that COMBIVENT nebuliser solution in unit dose vials (UDV) be administered via a mouth piece. If this is not available and a nebuliser mask is used, it must fit properly.
Systemic effects: In the following conditions COMBIVENT should only be used after careful risk/benefit assessment, especially when doses higher than recommended are used: insufficiently controlled diabetes mellitus, recent myocardial infarction, severe organic heart or vascular disorders, hyperthyroidism, phaeochromocytoma, risk of narrow-angle glaucoma, prostatic hypertrophy or bladder-neck obstruction.
Cardiovascular effects: Cardiovascular effects may be seen with sympathomimetic drugs, including COMBIVENT. There is some evidence from post-marketing data and published literature of rare occurrences of myocardial ischaemia associated with salbutamol. Patients with underlying severe heart disease (e.g. ischaemic heart disease, tachyarrhythmia or severe heart failure) who are receiving salbutamol for respiratory disease, should be warned to seek medical advice if they experience chest pain or other symptoms of worsening heart disease. Attention should be paid to assessment of symptoms as dyspnoea and chest pain, as they may be of either respiratory or cardiac origin.
Hypokalaemia: Potentially serious hypokalaemia may result from beta2-agonist therapy. Additionally, hypoxia may aggravate the effects of hypokalaemia on cardiac rhythm. In such situations, monitoring of serum potassium levels is recommended.
Gastro-intestinal motility disturbances: Patients with cystic fibrosis may be more prone to gastro-intestinal motility disturbances.
Dyspnoea: In the case of acute, rapidly worsening dyspnoea patients should be advised to consult a physician immediately.
Interference with laboratory tests or other diagnostic measures: The use of COMBIVENT may lead to positive results with regards to salbutamol in tests for nonclinical substance abuse, e.g. in the context of athletic performance enhancement (doping).
Driving and Using Machines: No studies on the effects on the ability to drive and use machines have been performed.
However, patients should be advised that they may experience undesirable effects such as dizziness, accommodation disorder, mydriasis and blurred vision during treatment with COMBIVENT. Therefore, caution should be recommended when driving a car or operating machinery.
Pregnancy: The safety of COMBIVENT during human pregnancy has not been established. The inhibitory effect of COMBIVENT on uterine contraction should be taken into account. The benefits of using COMBIVENT during a confirmed or suspected pregnancy must be weighed against possible hazards to the unborn child. The usual precautions regarding the use of drugs in pregnancy, especially during the first trimester, should be observed.
For ipratropium bromide, nonclinical studies have shown no embryotoxic or teratogenic effects following inhalation or intranasal application at doses considerably higher than those recommended in man. For salbutamol sulphate, non-inhalation nonclinical studies did not indicate direct or indirect harmful effects unless the inhalation Maximum Recommended Human Daily Dose (MRHDD) was exceeded (see Pharmacology: Toxicology under Actions).
Lactation: It is not known whether ipratropium bromide and salbutamol sulphate are excreted in breast milk. It is considered unlikely that ipratropium bromide would reach the infant to an important extent, especially when administered by inhalation. However, because many drugs are excreted in breast milk, caution should be exercised when COMBIVENT is administered to nursing mothers.
Fertility: No studies on the effect on human fertility have been conducted for COMBIVENT. Clinical data on fertility are neither available for the combination of ipratropium bromide and salbutamol sulphate nor for each of the two components of the combination.
Nonclinical studies performed with ipratropium bromide and salbutamol showed no adverse effect on fertility (see Pharmacology: Toxicology under Actions).
Summary of the safety profile: Many of the listed undesirable effects can be assigned to the anticholinergic and beta2-sympathomimetic properties of COMBIVENT. As with all inhalation therapy COMBIVENT may show symptoms of local irritation.
The most frequent side effects reported in clinical trials were headache, throat irritation, cough, dry mouth, gastro-intestinal motility disorders (including constipation, diarrhoea and vomiting), nausea, and dizziness.
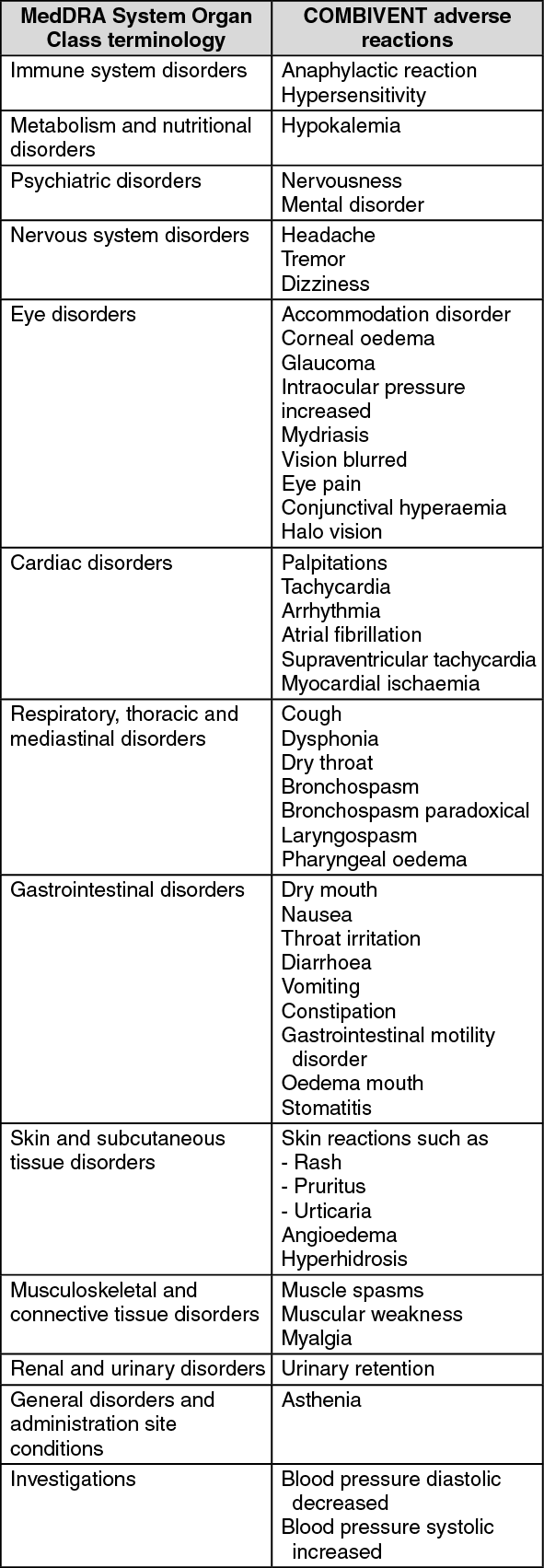
Tabulated summary of adverse reactions: The following adverse reactions have been reported during use of COMBIVENT in clinical trials and during the post-marketing experience. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The chronic co-administration of COMBIVENT with other anticholinergic drugs has not been studied. Therefore, the chronic co-administration of COMBIVENT with other anticholinergic drugs is not recommended.
The concurrent administration of xanthine derivatives as well as other beta-adrenergics and anticholinergics may increase the side effects.
Beta2-agonist induced hypokalaemia may be increased by concomitant treatment with xanthine derivatives, glucocorticosteroids and diuretics. This should be taken into account particularly in patients with severe airway obstruction.
Hypokalaemia may result in an increased susceptibility to arrhythmias in patients receiving digoxin.
It is recommended that serum potassium levels are monitored in such situations.
A potentially serious reduction in bronchodilator effect may occur during concurrent administration of beta-blockers.
Beta2-adrenergic agonists should be administered with caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, since the action of beta-adrenergic agonists may be enhanced.
Inhalation of halogenated hydrocarbon anaesthetics such as halothane, trichloroethylene and enflurane may increase the susceptibility to the cardiovascular effects of beta-agonists.
Store below 30°C and protect from light.
R03AL02 - salbutamol and ipratropium bromide ; Belongs to the class of combination of adrenergics with anticholinergics, that may also include a corticosteroid. Used in the treatment of obstructive airway diseases.
Combivent UDV inhalation soln
(unit dose) 2.5 mL x 60 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
